
Today’s Dietitian
Vol. 18 No. 4 P. 18
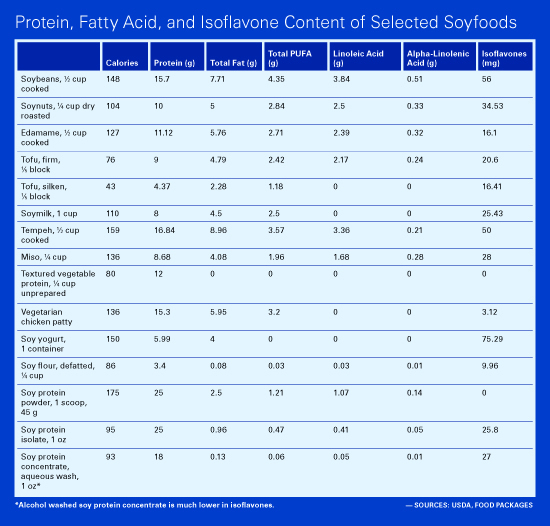
Evidence shows soyfoods can improve heart health due to their rich fatty acid, protein, and isoflavone content.
Diets that are predominantly based on plant foods have been associated with reduced risk of heart disease. This is most likely due to their lower saturated fat content and higher contents of fiber and beneficial phytochemicals, including antioxidants. According to recent research, incorporating soyfoods into plant-based diets may provide additional benefits. These foods have been linked to lower risk of heart disease not only because of their beneficial fatty acid profiles but also because of their protein and isoflavone content.
Soyfoods have a rich nutritional profile as well as a rich history, as they have been enjoyed by various cultures for hundreds of years.
Rich History
From both a culinary and nutritional standpoint, beans—including soybeans—are critical to the culinary traditions of populations consuming plant-based diets. In many Asian countries, soybeans and the foods made from them—tofu, soymilk, miso, tempeh, okara, and natto—have been important in diets for centuries. And they continue to play essential roles in the modern cuisine of these countries.
In Japan, tofu, miso, and natto are the most commonly consumed soyfoods.1 Soymilk, tofu, and processed soy products are frequent parts of meals in China, although the type and amount of soy consumed varies widely throughout the country.2 The fermented soy product tempeh is considered to be the national food of Indonesia, where it’s used in snacks or meals as a boiled or fried dish.3 Despite the popularity of tempeh in this country, however, almost one-half of all soy consumed in Indonesia is tofu.4
Although all beans are rich in protein, soybeans are exceptional for both their quality and quantity of this nutrient. One-half cup of cooked soybeans provides approximately 15 g protein, which is about twice the amount found in other legumes. Based on the protein digestibility-corrected amino acid score, the quality of soy protein is equivalent to protein from animal foods and is higher than other plant proteins. Many soyfoods also are good sources of calcium, making a potentially important contribution to bone health in populations where dairy foods are seldom consumed. They also provide a significant source of iron, which is present in a form that appears to be well absorbed even in the presence of phytate.5
In Western countries, soyfoods are increasingly popular as a way of exploring Asian cuisine and as a replacement for meat and dairy products among those eating plant-based diets. Tofu is used to replace eggs as breakfast items, meat or chicken in stir-fries, and cream or soft cheeses in recipes. Soymilk is a popular choice among people who prefer plant-based milks as a beverage or in cooking. The food industry has long used isolated and concentrated soy proteins as functional ingredients, and they’re important for producing meat analogs for vegetarians and others looking to reduce meat intake.
The popularity of soyfoods has been due to their rich nutrient content and versatility. A new focus of interest, however, which dates to the early 1990s, is the health effects of phytonutrients such as isoflavones. These phytoestrogens may play a role in reducing cancer risk6 and may be useful in managing menopause symptoms.7
Although isoflavones also may have a role in protecting against heart disease, much of the focus in this area has returned to the macronutrient content of soybeans—namely, their protein and fatty acid composition.
Heart Disease Incidence and Soyfood Consumption
Three prospective epidemiologic studies have evaluated the association between soy intake and coronary heart disease (CHD) among women in Asia. In the Shanghai Women’s Health Study (SWHS), which includes 65,000 postmenopausal women, subjects in the fifth percentile for soy protein consumption had an 86% lower risk of nonfatal myocardial infarction than women in the lowest percentile.2 Among 40,462 women enrolled in the Japan Public Health Center-based (JPHC) study cohort,1 those who consumed soyfoods at least five times per week were one-third less likely to die of CHD compared with women who consumed soyfoods no more than two times per week. Frequent soy consumers also were less likely to have had a stroke.8
In contrast, there were no cardioprotective effects associated with soyfood consumption in the Singapore Chinese Health Study.9 Nor were soyfoods protective against heart disease in men in either the Shanghai Men’s Health Study10 or in the JPHC,8 suggesting that the effects of soy consumption on heart disease may be gender specific.
While the results from epidemiologic studies are somewhat conflicting regarding soyfood consumption and heart health, clinical research points to an intriguing relationship between certain components of soyfoods and markers of heart disease risk, including LDL cholesterol, blood pressure, and arterial health. Soy’s fatty acid, protein, and isoflavone content may all work toward improving heart health when soyfoods are included in diets.
Fatty Acids in Soyfoods
Soybeans are unique among legumes because of their high fat content. Whole soybeans are about 40% fat as a percentage of calories compared with just 4% fat in pinto beans. The fat content of foods made from soybeans varies considerably depending on whether the whole bean is used. Textured vegetable protein—which is typically made from defatted soy flour—is fat-free, while traditional soyfoods such as tofu, soymilk, and tempeh are closer in fat content to the whole soybean.
The fat from soyfoods is predominately polyunsaturated (~59%) and monounsaturated (~29%).11 Soybeans are among a handful of plant foods that provide both the essential omega-6 fat linoleic acid and the essential omega-3 fat alpha-linolenic acid. One-half cup of cooked soybeans provides between 25% and 35% of the requirement for alpha-linolenic acid.
Recent research shows that replacing saturated fat in the diet with polyunsaturated fat is far more effective at reducing CHD risk than replacing saturated fat with either monounsaturated fat or carbohydrate from whole grains.12 (Replacing saturated fat with carbohydrate from refined grains or added sugar doesn’t reduce risk at all.) There’s also evidence that the high linoleic and alpha-linolenic acid content of soybean oil may be especially helpful for reducing heart disease risk.13,14
Researchers from the University of Toronto estimated that when 25 g of soy protein from soyfoods replace 25 g of protein from commonly consumed sources of protein in the US diet, LDL cholesterol will decrease by approximately 4% because of the favorable change in the fatty acid composition of the diet.15
Soy Protein and LDL Cholesterol Levels
Their fatty acid profile makes soyfoods, like all plant foods, a potentially valuable part of heart-healthy diets. Their protein content, however, may make them unique among plant foods in protecting against heart disease.
In 1999, the FDA approved a health claim for soyfoods and heart disease based on the cholesterol-lowering effects of soy protein.16 Similar claims have been approved in more than 10 other countries since 1999.17 The most recent country to register a claim was Canada in 2014.18
The FDA established 25 g of soy protein per day as the intake threshold for cholesterol reduction. This is the amount found in about three servings of tofu or soymilk. Some but not all evidence suggests that lower amounts of soy protein may lower cholesterol.19
Meta-analyses of clinical trials published since 2005 indicate that soy protein lowers LDL cholesterol by 4% to 6%,15,20-23 which is similar to cholesterol-lowering effects of soluble fiber.24 Compared with drug intervention, this is a modest reduction, but it’s enough to produce meaningful protection from heart disease. Each 1% reduction in cholesterol is estimated to lower risk of CHD by 1% to 2%,25,26 suggesting that soy protein alone could reduce heart disease risk by anywhere from 4% to 12%.
Furthermore, soy protein has been shown to lower circulating triglyceride levels by approximately 5% to 10% without affecting HDL cholesterol and may, in fact, increase HDL cholesterol by 1% to 3%.20 This again may be clinically relevant since each 1% or 1-mg increase in HDL cholesterol lowers CHD risk by 2% to 3%.27 There’s some debate about whether or not elevated triglyceride levels alone predict heart disease risk.28 However, elevated postprandial triglyceride levels may be an important risk factor for heart disease; limited research suggests soy lowers this CHD risk factor.29
Health Benefits Beyond Serum Cholesterol
The magnitude of reduction in heart disease risk among women in studies like the SWHS and JPHC suggest that the coronary benefits of consuming soyfoods go beyond what would be expected from cholesterol reduction alone. Additional protection may come from effects of isoflavones on endothelial function.
A recent meta-analysis found that soy improved endothelial function in postmenopausal women but only in those who had impaired endothelial function at baseline.30 A second meta-analysis found modest beneficial effects of soy consumption on endothelial function whether or not endothelial function was impaired at enrollment.31
In the Women’s Isoflavone Soy Health study, carotid intima-media thickness (CIMT) progression was 16% lower in women consuming isoflavone-rich soy protein (containing 91 mg of isoflavones, or the amount in three to four servings of traditional soyfoods such as tofu, tempeh, or soymilk) compared with women consuming milk protein.32 While the results weren’t statistically significant, an interesting finding was that CIMT progression was reduced to a much greater extent in women who were in early menopause. This is consistent with the estrogen timing hypothesis, which maintains that exposure to estrogenlike compounds leads to dramatic reductions in heart disease risk when begun soon after menopause, but has less effect in later years.33
Several studies have shown that soy and/or isoflavones improve systemic arterial compliance, another measure of arterial health.34 Finally, soy may reduce LDL oxidation and increase LDL particle size, both of which can be expected to reduce risk of heart disease.35,36 However, study findings are limited and/or inconsistent regarding these factors.
Potential effects of soy isoflavones are intriguing since they could explain gender differences in outcomes from epidemiologic studies on soy and heart health. Particularly in studies where soy protein intake may have been too low to provide protection, women may have reaped benefits from isoflavone intake that weren’t relevant in male subjects.
Impact on Blood Pressure
Approximately one decade ago, the authors of a commentary published in the Canadian Medical Association Journal suggested that soy protein could be the next antihypertension agent.37 But it wasn’t until Harvard University researchers showed in 2007 that soy dramatically lowered blood pressure that the hypotensive effects of soy received widespread attention.38 In this study, 25 g of protein intake per day from soynuts lowered systolic and diastolic blood pressure by 9.9% and 6.8%, respectively, in hypertensive women, and by 5.2% and 2.9%, respectively, in normotensive women. A few years before that, Spanish researchers already had shown that soymilk (500 mL twice per day) had similar benefits, reducing blood pressure by 16 mm Hg to 18 mm Hg in comparison with cow’s milk.39
However, while four recently published meta-analyses of the clinical data found reductions in blood pressure with consumption of soy protein, the effects were much smaller.40-43 Since many of the trials that showed effects didn’t have blood pressure as a primary focus of the study, more research is needed to determine the relationship of soy consumption to blood pressure.
Soyfoods as Part of a Heart-Healthy Diet
Overall, what the research has found is that incorporating more legumes and other plant foods into diets is beneficial for reducing heart disease risk because of favorable changes in the fatty acid profile of the diet. Soyfoods can be an important part of this approach since they’re a good source of both essential fatty acids and are especially versatile as replacements for meat, dairy products, and eggs. In addition, research shows that soy protein lowers blood cholesterol levels and that soy consumption may improve blood pressure and arterial health.
The findings regarding soyfoods and heart health are encouraging, but reducing risk of heart disease requires a comprehensive approach, not the addition of a single food item. For example, the portfolio diet developed at the University of Toronto has had dramatic effects on blood cholesterol levels, reducing them by as much as 30%.44 The diet combines dietary factors such as heart-healthy fats, phytosterols, nuts, and fiber as well as 23 g of soy protein from foods such as soymilk, tofu, and soy-based meat substitutes for each 1,000 kcal consumed. Each of the major elements of the portfolio diet has been shown to independently lower cholesterol. Recently, this diet also has been found to lower blood pressure even more effectively than the DASH diet.45
More research is needed on some aspects of soyfoods and heart disease reduction such as the effects of soy isoflavones on certain risk factors. However, it’s clear that soyfoods can play a useful role in comprehensive approaches to heart health that include a healthful diet, exercise, and smoking cessation. About three servings per day of soyfoods will likely provide the amount of soy protein and isoflavones that have been found to be beneficial in studies.
— Virginia Messina, MPH, RD, is a writer and speaker on vegetarian and vegan diets for the public and health professionals. She’s coauthor of Vegan for Life, Vegan for Her, and Never Too Late to Go Vegan, as well as a textbook on vegetarian nutrition for dietitians. Her website is TheVeganRD.com.
References
1. Wakai K, Egami I, Kato K, et al. Dietary intake and sources of isoflavones among Japanese. Nutr Cancer. 1999;33(2):139-145.
2. Zhang X, Shu XO, Gao YT, et al. Soy food consumption is associated with lower risk of coronary heart disease in Chinese women. J Nutr. 2003;133(9):2874-2878.
3. Astuti M, Meliala A, Dalais FS, Wahlqvist ML. Tempe, a nutritious and healthy food from Indonesia. Asia Pac J Clin Nutr. 2000;9(4):322-325.
4. Purba MB, Lukito W, Wahlqvist ML, et al. Food intake and eating patterns of Indonesian elderly before the 1998 economic crisis. Asia Pac J Clin Nutr. 1999;8(3):200-206.
5. Lönnerdal B. Soybean ferritin: implications for iron status of vegetarians. Am J Clin Nutr. 2009;89(5):1680S-1685S.
6. Sarkar FH, Li Y. Soy isoflavones and cancer prevention. Cancer Invest. 2003;21:744-757.
7. Taku K, Melby MK, Kronenberg F, Kurzer MS, Messina M. Extracted or synthesized soybean isoflavones reduce menopausal hot flash frequency and severity: systematic review and meta-analysis of randomized controlled trials. Menopause. 2012;19(7):776-790.
8. Kokubo Y, Iso H, Ishihara J, et al. Association of dietary intake of soy, beans, and isoflavones with risk of cerebral and myocardial infarctions in Japanese populations: the Japan Public Health Center-based (JPHC) study cohort I. Circulation. 2007;116(22):2553-2562.
9. Talaei M, Koh WP, van Dam RM, Yuan JM, Pan A. Dietary soy intake is not associated with risk of cardiovascular disease mortality in Singapore Chinese adults. J Nutr. 2014;144(6):921-928.
10. Yu D, Zhang X, Xiang YB, et al. Association of soy food intake with risk and biomarkers of coronary heart disease in Chinese men. Int J Cardiol. 2014;172(2):e285-e287.
11. Slavin M, Kenworthy W, Yu LL. Antioxidant properties, phytochemical composition, and antiproliferative activity of Maryland-grown soybeans with colored seed coats. J Agric Food Chem. 2009;57(23):11174-11185.
12. Li Y, Hruby A, Bernstein AM, et al. Saturated fats compared with unsaturated fats and sources of carbohydrates in relation to risk of coronary heart disease: a prospective cohort study. J Am Coll Cardiol. 2015;66(14):1538-1548.
13. Farvid MS, Ding M, Pan A, et al. Dietary linoleic acid and risk of coronary heart disease: a systematic review and meta-analysis of prospective cohort studies. Circulation. 2014;130(18):1568-1578.
14. Ramsden CE, Zamora D, Leelarthaepin B, et al. Use of dietary linoleic acid for secondary prevention of coronary heart disease and death: evaluation of recovered data from the Sydney Diet Heart Study and updated meta-analysis. BMJ. 2013;346:e8707.
15. Jenkins DJ, Mirrahimi A, Srichaikul K, et al. Soy protein reduces serum cholesterol by both intrinsic and food displacement mechanisms. J Nutr. 2010;140(12):2302S-2311S.
16. Food labeling: health claims; soy protein and coronary heart disease. Food and Drug Administration, HHS. Final rule. Fed Regist. 1999; 64(206):57699-57733.
17. Xiao CW. Health effects of soy protein and isoflavones in humans. J Nutr. 2008;138(6):1244S-1249S.
18. Benkhedda K, Boudrault C, Sinclair SE, Marles RJ, Xiao CW, Underhill L. Food risk analysis communication: Health Canada’s proposal to accept a health claim about soy products and cholesterol lowering. Int Food Risk Anal J. 2014;4:22.
19. Nagata C, Takatsuka N, Kurisu Y, Shimizu H. Decreased serum total cholesterol concentration is associated with high intake of soy products in Japanese men and women. J Nutr. 1998;128(2):209-213.
20. Zhan S, Ho SC. Meta-analysis of the effects of soy protein containing isoflavones on the lipid profile. Am J Clin Nutr. 2005;81(2):397-408.
21. Harland JI, Haffner TA. Systematic review, meta-analysis and regression of randomised controlled trials reporting an association between an intake of circa 25g soya protein per day and blood cholesterol. Atherosclerosis. 2008;200(1):13-27.
22. Reynolds K, Chin A, Lees KA, Nguyen A, Bujnowski D, He J. A meta-analysis of the effect of soy protein supplementation on serum lipids. Am J Cardiol. 2006;98(5):633-640.
23. Anderson JW, Bush HM. Soy protein effects on serum lipoproteins: a quality assessment and meta-analysis of randomized, controlled studies. J Am Coll Nutr. 2011;30(2):79-91.
24. Brown L, Rosner B, Willett WW, Sacks FM. Cholesterol-lowering effects of dietary fiber: a meta-analysis. Am J Clin Nutr. 1999;69(1):30-42.
25. Law MR, Wald NJ, Thompson SG. By how much and how quickly does reduction in serum cholesterol concentration lower risk of ischaemic heart disease? BMJ. 1994;308(6925):367-372.
26. Law MR, Wald NJ, Wu T, Hackshaw A, Bailey A. Systematic underestimation of association between serum cholesterol concentration and ischaemic heart disease in observational studies: data from the BUPA study. BMJ. 1994;308(6925):363-366.
27. Boden WE. High-density lipoprotein cholesterol as an independent risk factor in cardiovascular disease: assessing the data from Framingham to the Veterans Affairs High-Density Lipoprotein Intervention Trial. Am J Cardiol. 2000;86(12A):19L-22L.
28. Cullen P. Evidence that triglycerides are an independent coronary heart disease risk factor. Am J Cardiol. 2000;86(9):943-949.
29. Santo AS, Santo AM, Browne RW, et al. Postprandial lipemia detects the effect of soy protein on cardiovascular disease risk compared with the fasting lipid profile. Lipids. 2010;45(12):1127-1138.
30. Li SH, Liu XX, Bai YY, et al. Effect of oral isoflavone supplementation on vascular endothelial function in postmenopausal women: a meta-analysis of randomized placebo-controlled trials. Am J Clin Nutr. 2010;91(2):480-486.
31. Beavers DP, Beavers KM, Miller M, Stamey J, Messina MJ. Exposure to isoflavone-containing soy products and endothelial function: a Bayesian meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2012;22(3):182-191.
32. Hodis HN, Mack WJ, Kono N, et al. Isoflavone soy protein supplementation and atherosclerosis progression in healthy postmenopausal women: a randomized controlled trial. Stroke. 2011;42(11):3168-3175.
33. Hodis HN, Mack WJ. A “window of opportunity:” the reduction of coronary heart disease and total mortality with menopausal therapies is age- and time-dependent. Brain Res. 2011;1379:244-252.
34. Pase MP, Grima NA, Sarris J. The effects of dietary and nutrient interventions on arterial stiffness: a systematic review. Am J Clin Nutr. 2011;93(2):446-454.
35. Jenkins DJ, Kendall CW, Connelly PW, et al. Effects of high- and low-isoflavone (phytoestrogen) soy foods on inflammatory biomarkers and proinflammatory cytokines in middle-aged men and women. Metabolism. 2002;51(7):919-924.
36. Desroches S, Mauger JF, Ausman LM, Lichtenstein AH, Lamarche B. Soy protein favorably affects LDL size independently of isoflavones in hypercholesterolemic men and women. J Nutr. 2004;134(3):574-579.
37. Cartagena AM. Soy protein: the next antihypertensive agent? CMAJ. 2005;173(5):486.
38. Welty FK, Lee KS, Lew NS, Zhou JR. Effect of soy nuts on blood pressure and lipid levels in hypertensive, prehypertensive, and normotensive postmenopausal women. Arch Intern Med. 2007;167(10):1060-1067.
39. Rivas M, Garay RP, Escanero JF, Cia P Jr, Cia P, Alda JO. Soy milk lowers blood pressure in men and women with mild to moderate essential hypertension. J Nutr. 2002;132(7):1900-1902.
40. Hooper L, Kroon PA, Rimm EB, et al. Flavonoids, flavonoid-rich foods, and cardiovascular risk: a meta-analysis of randomized controlled trials. Am J Clin Nutr. 2008;88(1):38-50.
41. Dong JY, Tong X, Wu ZW, Xun PC, He K, Qin LQ. Effect of soya protein on blood pressure: a meta-analysis of randomised controlled trials. Br J Nutr. 2011;106(3):317-326.
42. Liu XX, Li SH, Chen JZ, et al. Effect of soy isoflavones on blood pressure: a meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2012;22(6):463-470.
43. Taku K, Lin N, Cai D, et al. Effects of soy isoflavone extract supplements on blood pressure in adult humans: systematic review and meta-analysis of randomized placebo-controlled trials. J Hypertens. 2010;28(10):1971-1982.
44. Jenkins DJ, Kendall CW, Faulkner D, et al. A dietary portfolio approach to cholesterol reduction: combined effects of plant sterols, vegetable proteins, and viscous fibers in hypercholesterolemia. Metabolism. 2002;51(12):1596-1604.45. Jenkins DJ, Jones PJ, Frohlich J, et al. The effect of a dietary portfolio compared to a DASH-type diet on blood pressure. Nutr Metab Cardiovasc Dis. 2015;25(12):1132-1139.