
Today’s Dietitian
Vol. 19, No. 7, P. 36
Hypoglycemia, or low blood glucose, is a challenging and potentially life-threatening condition that people with diabetes often face. According to the American Diabetes Association and Endocrine Society Workgroup, hypoglycemia is defined as all episodes of an abnormal low plasma glucose concentration (with or without symptoms) that expose an individual to harm. For people with diabetes, this means a glucose level of 70 mg/dL or below.1 Hypoglycemia is common in diabetes and considered a dangerous complication requiring immediate attention.
Population-based data show that 30% to 40% of people with type 1 diabetes experience an average of one to three episodes of severe hypoglycemia (requiring the assistance of another) each year. Event rates of hypoglycemia in insulin-treated type 2 diabetes are approximately 30% of that in type 1 diabetes (35 vs 115 episodes per 100 patient-years). Older individuals are at increased risk of adverse events due to age-related adaptive response to low blood glucose and changes in food intake. Therefore, hypoglycemia prevention should be addressed in this population.2
Low blood glucose levels can wreak havoc on a person’s overall physical and emotional health and reduce one’s ability to properly manage their daily diabetes self-care management. The brain requires adequate glucose (or sugar) for fuel, and without sufficient energy, even simple daily tasks become challenging. Interestingly, brain and nerve cells don’t require the hormone insulin to absorb sugar. These cells have built-in transporters that move sugar across the cell membrane without insulin. However, low blood glucose eventually will cause confusion and lead to impaired decision making.
Blood glucose levels may fall into a dangerously low range for a variety of reasons, including taking too much insulin or other blood glucose-lowering medications, missing a meal, or excessive physical activity. Low blood glucose can lead to serious health problems, either from an inadequate supply of glucose to the brain, or possible trauma due to confusion or loss of consciousness (such as when driving or operating machinery). Anyone who depends on insulin to manage his or her diabetes and stay alive probably has dealt with hypoglycemia at one point or another.
Stress hormones are released once blood glucose levels drop to a low level. The brain signals the adrenal gland, which releases the hormone adrenaline. Adrenaline, in turn, signals the liver to secrete sugar into the bloodstream, which in turn blocks the usual action of insulin. Adrenaline production causes shaking, hunger, rapid heartbeat, and feelings of anxiety. These also are typical hypoglycemia symptoms.
If blood glucose continues to drop, one loses the ability to think clearly and may become dizzy and weak. A drop in blood glucose can make reading comprehension nearly impossible. In addition, low blood glucose may cause blurred vision, which may cause disorientation. This entire process makes rational thought, work, school, and activities such as driving extremely difficult. The signs and symptoms of hypoglycemia may be different for each person (see sidebar).
Causes and Treatment
Medication Mix-Ups
According to Francine Kaufman, MD, chief medical officer and vice president of global medical, clinical, and health affairs at Medtronic, one of the world’s largest medical technology, services, and solutions companies, and former president of the American Diabetes Association, there are several factors that may lead to diabetes-related hypoglycemia: errors in insulin or medication doses, mistakes in calculating the amount of insulin required to cover a meal or snack, mixing up insulin (ie, taking morning insulin at night or vice versa), or drinking alcohol on an empty stomach. “Long bouts of exercise or drinking alcohol without eating enough food can send your blood glucose falling to dangerous levels,” Kaufman says, adding that people with diabetes should prepare for delayed mealtimes or other possible scheduling conflicts following their insulin dosage (for example when eating out) to help prevent hypoglycemia.3
Adjust Target Blood Glucose Range
According to Henry Anhalt, DO, a pediatric endocrinologist and chief medical officer for T1D Exchange, a Boston-based nonprofit organization dedicated to accelerating research and improving type 1 diabetes outcomes, surveillance data often are inadequate and unreliable for capturing the real problem of hypoglycemia. Young children and the elderly are at significant risk of adverse outcomes due to hypoglycemia, Anhalt says. “It may be prudent to adjust blood glucose goals to higher targets for 48 to 72 hours to help restore autonomic functions and reduce the emotional toll low blood glucose levels take on our patients,” Anhalt says. He also points out the complication of significant cardiovascular disease in people who experience hypoglycemia. “Hypoglycemia can lead to arrhythmias, ischemia, and death,” he continues. “The emotional and physical toll of recurrent low blood glucose must inspire us as clinicians to speak with people with diabetes without any preconceived judgment, and encourage patients to be honest with us, so we can adjust medications as needed. Physicians should refer our patients with diabetes to registered dietitians to assist with meal planning and snack adjustments to help combat the issue of hypoglycemia.”
Avoid Fixed Insulin Ratios
Gary Scheiner, MS, CDE, owner of Integrated Diabetes Services, and the 2014 American Association of Diabetes Educators diabetes educator of the year, has lived with type 1 diabetes for 32 years. Scheiner suggests matching a patient’s insulin program to actual needs or individual requirements. “The peaks and valleys in your insulin should coincide with the peaks and valleys in your blood glucose levels. This usually means utilizing a basal/bolus insulin approach—(a long-acting insulin glargine, detemir, degludec, U-300 glargine) working at a low level throughout the day and night, and rapid-acting insulin at each meal or snack, or an insulin pump. Use of NPH (intermediate insulin) or premixed insulin (70/30) during the day can set a person up for lows if something changes in their routine (such as extra physical activity or a delayed meal). Also, at mealtimes, it’s better to use a rapid-acting insulin analog (eg, aspart, glulisine, or lispro) than regular insulin because the rapid analogs finish working earlier and are less likely to cause premeal lows.”4
The 15/15 Rule and Beyond
Glucose or simple carbohydrate is the preferred treatment for the conscious individual with hypoglycemia. Many dietitians and diabetes educators teach the 15/15 rule for treatment of low blood glucose.
Immediate treatment with carbohydrates is essential for low blood glucose. The standard treatment for a blood glucose level below 70 mg/dL (3.9 mmol/L) is to treat with 15 g carbohydrate. Recheck blood sugar in 15 minutes. If blood glucose is still below 70 mg/dL, treat with an additional 15 g carbohydrate using the following strategies:
• three to four glucose tablets;
• 4 to 6 oz fruit juice or regular soft drink;
• 6 oz regular soda (not sugar-free);
• 8 oz (1 cup) sports drink (not sugar-free);
• 1 T sugar or five small sugar cubes; or
• 1 T syrup or honey.
Repeat until blood glucose level returns to target range.
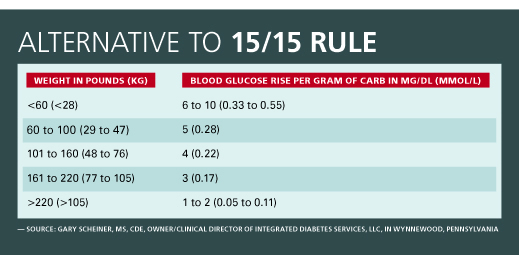
While the 15/15 rule is a standard reference used to treat hypoglycemia, many experienced practitioners choose to use a more individualized treatment approach. Scheiner says carbohydrate grams should be based on body weight, rather than using 15 g carbohydrate as a standard for children and adults.
“The bigger you are, the more carbohydrate it takes to raise blood glucose. This is due to the fact that bigger people have more blood volume into which the glucose will dissolve. Every gram of carb will raise a small child’s blood glucose much more than that of a fully grown adult,” Scheiner says. (See table below for an alternative to the 15/15 rule.)
Don’t Depend on Protein
Often, patients are advised to add protein to the carbohydrate to prevent late onset hypoglycemia. Marion J. Franz, MS, RD, LD, CDE, a nutrition/health consultant with Nutrition Concepts by Franz, an organization that serves the health and dietetics food stores industry in Edina, Minnesota, and an author of numerous books about nutrition and diabetes, debunks this long-held notion. “Although nonessential amino acids undergo hepatic gluconeogenesis, peripheral glucose concentrations don’t increase after protein ingestion. Protein does not contribute to sustained glucose elevations, slow the absorption of carbohydrate, or help in the treatment of hypoglycemia.”5,6
Toby Smithson, MSNW, RDN, LDN, CDE, author of Diabetes Meal Planning & Nutrition for Dummies and a spokesperson for the Academy of Nutrition and Dietetics, has managed her own type 1 diabetes for more than four decades. She says she keeps a variety of snacks on hand to always be prepared for the expected or unexpected. “I carry snacks that are carbohydrates like hard candy, glucose tabs, or dried fruit to treat hypoglycemia, and stay clear from snacks that contain protein to treat my lows. I will carry sustaining snacks like nutrition bars and nuts for in between meals,” Smithson says.
Consider Continuous Glucose Monitoring
It’s important to speak with patients about the significance of frequent blood glucose monitoring. These vital data can be used to individualize meal plans, exercise programs, insulin regimes, and medications. Discuss available technology, including sensors, meters, and continuous glucose monitors (CGMs) to help achieve positive outcomes. CGMs have built-in alerts, which can show lowering blood glucose trends.
Keep Glucagon on Hand
When glucose levels are severely low, the person may not be able to swallow carbohydrate-containing food, and intramuscular glucagon will be required. Glucagon 1 mg should be administered intramuscularly or subcutaneously. It’s essential for parents, caregivers, spouses, family members, or roommates to learn how to properly use glucagon. Glucagon kits include prefilled syringes, as well as diluting fluid. After glucagon administration, normal plasma glucose levels may return in approximately 10 to 15 minutes. The patient may experience nausea or vomiting as a side effect from the glucagon. Unfortunately, glucagon may not be effective if the patient consumed a large amount of alcohol. Always call 911 if the individual is experiencing severely low blood glucose, although you still may have to administer glucagon.
Wear Medical Alert Identification
Moreover, it’s vitally important to educate patients about the importance of wearing a medical alert bracelet or other form of identification if they have diabetes. If they become hypoglycemic, confused, or disoriented, they may not be able to properly treat their low blood glucose. A medical alert bracelet is the first thing medical professionals look for when they suspect hypoglycemia or are trying to differentiate low blood glucose from intoxication, because the signs at first glance may appear to be similar.
Fine-Tune Mealtime and Timing of Meals
If patients are taking intermediate or long-acting insulin, they can better manage blood glucose levels by eating on a consistent schedule. If meals are significantly delayed (eg, late service when dining out or a traffic jam coming home from work), hypoglycemia can result. Dietitians should advise their patients to carry a carbohydrate-containing snack with them, in case their usual meal is delayed, to prevent an unwanted drop in blood glucose. Although foods high in fiber are healthful and should be included in meal planning, they shouldn’t be used to raise plummeting blood glucose levels.
Educate Family, Friends, and Coworkers
Advise patients to educate those around them about diabetes and hypoglycemia symptoms. Knowing the symptoms and treatment for hypoglycemia can alert friends, family, and coworkers to take immediate action. Remind patients to keep glucose tablets or another source of carbohydrate on hand to treat low blood glucose levels. Dietitians and diabetes educators always should keep glucose tablets in the office, and encourage blood glucose monitoring during sessions. This allows for an open discussion about managing daily diabetes care and preparedness for emergency situations.
Hypoglycemia Unawareness
In some circumstances, there are patients who are unaware that they’re having a hypoglycemic episode. Hypoglycemia unawareness is a condition that affects approximately 40% of people with type 1 diabetes, and this can have potentially deadly consequences.7 If a person with diabetes has suffered from hypoglycemia for many years, their brain may no longer properly detect mild low blood glucose levels and fail to produce an adrenaline or stress hormone response to produce the usual hypoglycemia warning signs. While normally a person may feel low blood glucose symptoms, lack of the stress response hormones causes an absence of physical symptoms such as shaking and sweating. It’s increasingly likely that the more serious issues, such as confusion, may not occur until blood glucose has dipped to a dangerously low level.
Anthony McCall, MD, PhD, an endocrinologist at the University of Virginia, says, “People with hypoglycemia unawareness often state that they’re OK because they don’t feel so bad. In fact, that’s when things become very dangerous.” McCall points out that older adults may be eating less and taking the same amount of insulin, which may increase their risk of low blood glucose levels. People suffering from hypoglycemia unawareness may experience very strange behavior, including extreme anger or irritability, explosive emotions such as inappropriate laughter, or irrational thought.
The problem of hypoglycemia unawareness may be caused by frequent low blood glucose, a rapid drop in blood glucose, having diabetes for many years (due to the lack of stress hormone production), excessive alcohol consumption, or use of medications such as beta-blockers prescribed for high blood pressure or heart disease. If too much alcohol is consumed, the liver is blocked from producing the glucose needed to raise blood glucose. In addition, free fatty acid release is blocked, so fuel for energy is limited. As previously discussed, glucagon administration may be needed.
Nocturnal hypoglycemia unawareness also is a major concern, as episodes may be connected to impaired counter regulatory-hormonal responses, and symptoms may go undetected. CGMs can help identify hypoglycemia unawareness during sleep and alert the person with diabetes to a dip in blood glucose during the overnight hours.8
The best advice for reversing hypoglycemia unawareness is to avoid frequent low blood glucose levels. This can be best accomplished by checking blood glucose levels often and consider wearing a CGM. Glucose meters should be easily accessible at home, work, or school. Moreover, matching your patients’ insulin to their lifestyle, speaking with their health care provider about target blood glucose levels, and improving self-care behaviors when possible are vital to monitoring this potentially life-threatening issue.
Prevention of Further Episodes
The one thing that’s predictable about diabetes is that it’s an incredibly unpredictable disease. So while it may be challenging for patients to prevent all future hypoglycemic episodes, evaluation of their current diabetes management plan should be addressed to reduce large fluctuations in blood glucose levels. Frequent blood sugar monitoring, exercising earlier in the day, follow-up with an endocrinologist or health care provider, and visits with a dietitian and certified diabetes educator are recommended. In addition, encouraging patients to enroll in approved diabetes self-care education programs (which may be covered by insurance) is key, as they provide much-needed support for those struggling with daily diabetes self-care management and offer peer support for problems associated with hypoglycemia or blood glucose fluctuations.
— Susan Weiner, MS, RDN, CDE, CDN, is the owner of Susan Weiner Nutrition, PLLC, and was named the 2015 AADE Diabetes Educator of the Year. She’s the coauthor of The Complete Diabetes Organizer: Your Guide to a Less Stressful and More Manageable Diabetes Life and Diabetes: 365 Tips for Living Well.
References
1. Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. J Clin Endocrinol Metab. 2013;98(5):1845-1859.
2. Sircar M, Bhatia A, Munshi M. Review of hypoglycemia in the older adult: clinical implications and management. Can J Diabetes. 2016;40(1):66-72.
3. Kaufman FR, ed. Medical Management of Type 1 Diabetes. 6th ed. Alexandria, VA: American Diabetes Association; 2012.
4. Scheiner G. Think Like a Pancreas: A Practical Guide to Managing Diabetes with Insulin. 2nd ed. Boston, MA: Da Capo Press; 2011.
5. Franz MJ, Evert AB. Medical nutrition therapy for diabetes mellitus and hypoglycemia of nondiabeteic origin. In: Mahan LK, Raymond JL. Krause’s Food & The Nutrition Care Process. 14th ed. St. Louis, MO: Elsevier; 2017:586-618.
6. Pastors JG, Franz MJ. Effectiveness of medical nutrition therapy in diabetes. In: Franz MG, Evert AB, ed. American Diabetes Association Guide to Nutrition Therapy for Diabetes. 2nd ed. Alexandria, VA: American Diabetes Association; 2012:1-18.
7. Martín-Timón I, Del Cañizo-Gómez FJ. Mechanisms of hypoglycemia unawareness and implications in diabetic patients. World J Diabetes. 2015;6(7):912-926.
8. Zijlstra E, Heise T, Nosek L, et al. Continuous glucose monitoring quality of hypoglycaemia detection. Diabetes Obes Metab. 2013;15(2):130-135.
SIGNS AND SYMPTOMS OF HYPOGLYCEMIA
• Shakiness, nervousness, or anxiety
• Sweating, chills, and clamminess
• Irritability or impatience
• Confusion
• Rapid/fast heartbeat
• Lightheadedness or dizziness
• Hunger and nausea
• Sleepiness
• Blurred/impaired vision
• Tingling or numbness in the lips or tongue
• Headaches, weakness
• Fatigue
• Anger
• Stubbornness or sadness
• Lack of coordination
• Nightmares
• Seizures
• Unconsciousness
* Note: It’s possible for these symptoms to occur with a blood glucose reading above 70 mg/dL due to a rapid decline in blood sugar from a hyperglycemic or high blood sugar state.— Source: http://professional.diabetes.org/pel/hypoglycemia-english